“A state of anxiety in response to perceived negative evaluation by others, concerning the performance of a procedural (surgical) task”
Introduction
Performance Anxiety (PA) has been documented in a number of settings, often affecting those with specialised skills, including athletes and musicians. While the performance arts and sporting communities have become more open to the recognition and management of performance anxiety over the past decade, the surgical community remains somewhat reticent, despite anecdotal evidence of its prevalence.
Our first project aims determine whether, and to what extent, performance anxiety affects surgeons (trainees and consultants) in the UK. Identification of performance anxiety among surgeons and the development of suitable coping strategies would be hugely beneficial for both surgeons and their patients. We hope to develop strategies to help support surgeons and optimise surgical performance.
How can anxiety affect performance
Performance anxiety can affect anyone, even those with specialist skills. A survey of 56 orchestras found that 70% of musicians experience anxiety excessive enough to impair performance (James, 1998) and a meta-analysis of 48 studies looking at anxiety in competitive sport for a significant association between greater levels of anxiety and poorer performance outcomes (Woodman & Hardy, 2003).
In addition to impact on performance is can affect the mental health of individuals. Importantly, we know that there is burnout amongst medics and surgeons.
How does performance anxiety differ from other performance related responses (in brief)?
Anxiety:
- Emotional response
- Associated with feelings of fear or dread
Stage fright:
- Can be thought of for a synonym for performance anxiety
Worry:
- A cognitive process
- Often takes the form of “what if?” thought
Stress:
- Can be thought as the psychological response to pressures and the body’s response to it
- Occurs when perceived demands are greater than perceived resources to cope
How and why does anxiety affect performance:
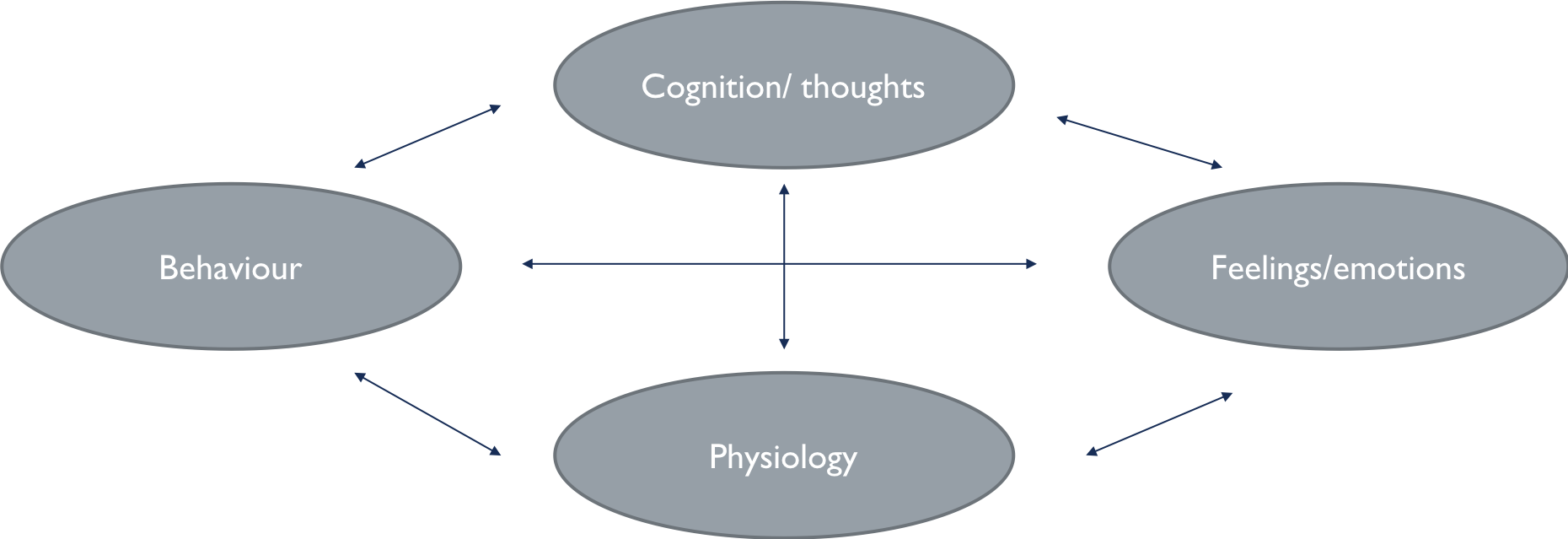
Feelings/ emotion = anxiety
Physiology:
- Anxiety is associated with (evolutionarily adaptive) autonomic nervous system changes:
- “Stress response” (adrenaline, cortisol etc). E.g. increased heart rate, nausea, sweating & shaking
- Prepares for a fight, flight or freeze response to threat cues
- Similar physiological response to an immediate threat (e.g. a tiger) and a perceived social threat (e.g. negative judgement from others)
- A level of physiological arousal can be helpful in certain situations (being chased by a tiger). However, arousal in surgery has been associated with increased error rates and poor economy of movement (Arora et al., 2010)
Cognition:
- Anxiety is associated with the allocation of attention to threat-related stimuli (Eysenck et al., 2007)
- Impairs ability to inhibit attention towards threat and shift attention to target stimuli
- E.g. it is hard not to focus on negative thoughts about the outcome of surgery and/or physiological symptoms and hard to shift attention the task at hand (performing the operation!)
- Decrease in processing efficiency (speed of information processing/speed of completing a task)
- When cognitive demands are already high, anxiety leads to an impairment in performance
Behaviour:
- Some ‘behaviours’ can be helpful
- Skill establishment = an increase of movement automacityas a result of practice (Carson & Collins, 2016)
- Practicing surgical task is becoming increasingly difficult with reductions in training time within rotas
- Some rituals have been shown to reduce anxiety and improve performance (Brooks et al., 2016)
- Distracting
- Increases sense of control
- Externalise the focus of attention
- Impact of such behaviour in surgery is unknown
Perfectionism
- There is a paradox between perfectionism and performance.
- An elite performer needs to strive for (near) perfection
- This can lead to greater skill-establishment
- However, perfection has been associated with greater anxiety (& worse performance)
What can we do to help?
We don’t know!
- CBT is most studied modality of intervention in music (Burin & Osorio, 2016)
- Reductions in Performance Anxiety
- Improvements in performance
- Increased confidence
- BUT – some small sample sizes, and not all studies find improvements
- Beta-blockerscan manage the somatic symptoms of anxiety (Kenny, 2005)
- BUT – anxiolytic medication may impact on fine motor control (Burin & Osorio, 2017)
- Mindfulness-based interventions in sport (e.g. cycling & running)
What we are doing:
We have developed a survey to help establish the role of performance anxiety and perfectionism in UK surgeons. We have designed a novel surgical performance anxiety inventory and a surgical perfectionism inventory which we use along side more probing questions regarding the possible impact of performance anxiety on individuals and the wider surgical community. In addition we collect demographic data and include inventors for trait anxiety and perfectionism.
The survey has been piloted and will go live in January 2019.
Study sponsor: Oxford University Hospitals NHS Trust
IRAS project ID: 214791
Funding: ASiT Surgical Training Research Grant
Participants:
Inclusion criteria: All surgeons in the UK, including consultants, fellows, staff grade/associate specialists and specialty doctors and trainees (ST1 onwards)
Exclusion criteria: Foundation year doctors
Please find the national survey at this link:
https://surveyhero.com/c/SurgicalPerformanceAnxietyNationalSurvey